1. Nº 57 .1 6 Madrid, 29 de junio de 2016 SALARIO MÍNIMO FRANCÉS. CERTIFICADO OFICIAL A menos de 48 de la entrada en vigor de la ley Macron para el transporte terrestre, las autoridades francesas han elevado por fin a definitivo el modelo de "Certificado de desplazamiento" que todos los conductores afectados deberán llevar consigo. Lo puede encontrar en este enlace: http://www.developpement- durable.gouv.fr/IMG/pdf/Attestation_de_detachement_d _un_travailleur_roulant_ou_naviguant_dans_le_cadre_de _l_execution_d_une_prestation_de_services_par_une_ent reprise_de_transport_.pdf Permite su cumplimentación informática. Lo enviamos también como anexo para comodidad de consulta. C/ Príncipe de Vergara, 7 4, 3 planta - 28006 MADRID Tlf.: 91 451 48 01 / 07 – Fax: 91 395 28 23 E-mail: astic@astic.net Nota: Prohibida la edición, distribución y puesta en red, total o parcial, de esta i nformación sin la autorización de A.S.T.I.C.
5. N– Modèle 1 – Annexe Annexe Appendix INFORMATIONS RELATIVES AU SALARIE ROULANT OU NAVIGA NT DETACHE Information relating to the mobile posted worker Cette annexe doit être complétée par l’employeur du salarié roulant ou navigant détaché en France, qu’ il soit ressortissant de l’Union européenne ou d’un Etat ti ers. The employer must complete this appendix for the mo bile worker posted in France, whether he is a Community or third-country national. Nom : __________________________________ Prénom: _____________________________________ Name: First name: Date de naissance : ________________ Lieu de naissa nce (ville et pays) : ________________________ Date of birth : Place of birth (town and country) : Nationalité : _______________ Nationality : Adresse de résidence habituelle : _______________ _____________________________________________ Address of ordinary residence : ___________________________________________________ ____________________________________ ___________________________________________________ ____________________________________ Date de signature du contrat de travail : _________ ______ Date of signature of work contract : Droit du travail applicable au contrat de travail : Labor law applicable to the work contract : ___________________________________________________ __ Qualification professionnelle : ___________________ ____________ Professional qualification : Taux de salaire horaire brut (converti en euros le cas échéant) : _____________________________ ___________________________________________________ _____________________________ Gross hourly wage (in €)
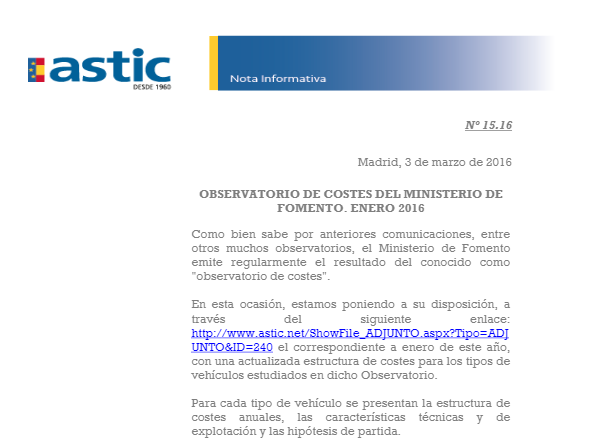
2. N– Modèle 1 – Annexe Ministère chargé du travail ATTESTATION DE DETACHEMENT Attestation relating to the posting of a worker DÉTACHEMENT D’UN TRAVAILLEUR ROULANT OU NAVIGANT DANS LE CADRE DE L’EXÉCUTION D’UNE PRESTATION DE SERVICES PAR UNE ENTREPRISE DE TRANSPORT POSTING OF A ROAD AND INLAND WATERWAY TRANSPORT MOB ILE WORKER IN THE FRAMEWORK OF THE PROVISION OF SERVICES BY A TRANSPO RT COMPANY N° xxxxx*xx Modèle 1 A remplir par l’employeur To be filled out by the employer Article R.1331-2 du code des transports Cette attestation est valable pour une durée maxima le de six mois à compter de sa date d’établissement This attestation is valid for a maximum period of s ix months after its date of issue Le formulaire d’attestation est établi en deux exem plaires dont l’un est remis au salarié détaché afin d’être conservé à bord du moyen de transport avec lequel e st assuré le service et l’autre est détenu par l’en treprise d’accueil du salarié roulant ou navigant détaché. The attestation form is drawn up in two copies, one is given to the posting worker to be kept in the v ehicle which the service is provided with, the other is kept by the borrowing company of the road or inland waterway tr ansport mobile worker. Veuillez remplir toutes les rubriques Please complete all headings EMPLOYEUR (employer) Nom ou raison sociale : ___________________________________________________ ____ Business name : Forme juridique de l’entreprise : _______________________________________________ Legal form Adresse complète dans le pays d’établissement (n°, voie, ville et pays): _______________________ ____ Full address in country of establishment (number, s treet, postal code, town and country): ___________________________________________________ ___________________________________ ___________________________________________________ ___________________________________ ___________________________________________________ ___________________________________ N° de téléphone : _______________________ Telephone number: Courriel :_________________________________________ _____________________________________ email : Références d’immatriculation au registre électroniq ue national des entreprises de transport par route prévu par l’article 16 du règlement européen (CE) n ° 1071/2009 du 21 octobre 2009 : ___________________________________________________ ___________________________________ Registration number in the national electronic regi ster of road transport undertakings (regulation (EC) n°1071/2009 of 21 october 2009) NOM(S) DU/DES ORGANISME(S) DE RECOUVREMENT DES COTI SATIONS DE SÉCURITÉ SOCIALE Name(s) of body/bodies collecting social security c ontributions ___________________________________________________ ___________________________________ ___________________________________________________ ___________________________________ 15553*01
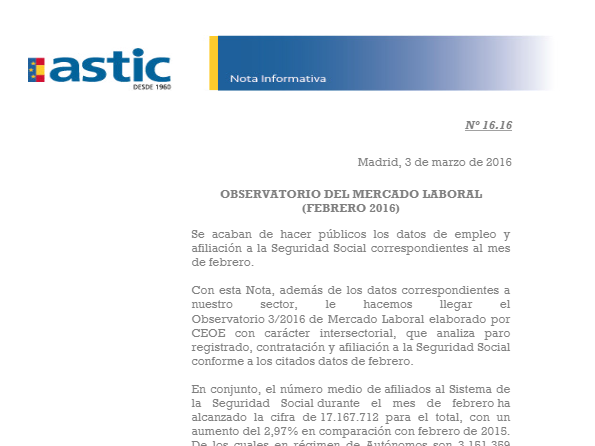
3. N– Modèle 1 – Annexe DIRIGEANT(S) DE L’ENTREPRISE Directors(s) Identité du dirigeant de l'entreprise : Identity of the company’s director: Nom : __________________________________ Prénom: ____________________________________ Name: First name: Date de naissance : ________________ Lieu de naissa nce (ville et pays) : _______________________ Date of birth : Place of birth (town and country) : Le cas échéant, identité des autres dirigeants : __ _____________________________________________ Identity of others directors, when applicable : REPRÉSENTANT EN FRANCE DE L’ENTREPRISE Company’s representative in France Identité du représentant en France : Identity of representative in France for the period of the service : Nom ou raison sociale (le cas échéant) : ___________ __________________________________________ Name or Business name (when appropriate) : Prénom : __________________ First name : Adresse complète postale en France (n°, voie, code postal et ville) : ______________________________ Full address in France (street number, postal code, town): ___________________________________________________ ___________________________________ ___________________________________________________ ___________________________________ ___________________________________________________ ___________________________________ N° de téléphone : _______________________ Telephone number: Courriel :_________________________________________ _____________________________________ Email : FRAIS DE VOYAGE, DE NOURRITURE ET, LE CAS ECHEANT, D’HEBERGEMENT ENGAGÉES PAR JOUR DE DÉTACHEMENT Travel, Meals and Lodging expenses per day of posti ng Frais de voyage (cocher la case correspondante) : Travel costs (Tick the relevant box) : □ Prise en charge directe par l’employeur Directly paid by the employer : □ Remboursement des frais avancés par le travailleur Reimbursement of expenses advanced by the worker : Préciser son montant (en euros) : ____________ Specify the amount of the reimbursement, in € : □ Versement d’une somme forfaitaire Lump-Sum payement : Préciser son montant (en euros) : ____________ Specify the amount of the lump-sum, in € :
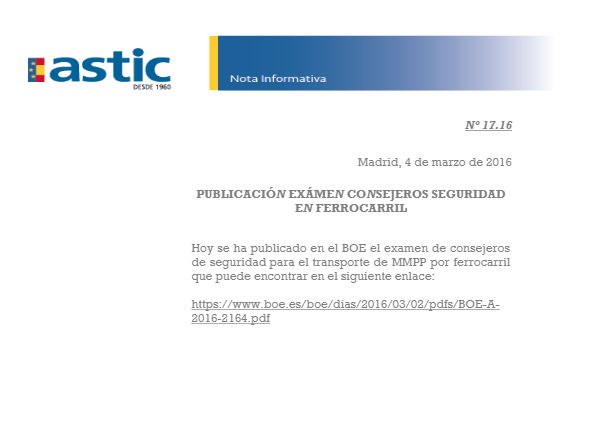
4. N– Modèle 1 – Annexe Frais de nourriture (cocher la case correspondante) : Meals expenses (check the relevant box) : □ Prise en charge directe par l’employeur Directly paid by the employer : □ Remboursement des frais avancés par le travailleur Reimbursement of expenses advanced by the workers : Préciser son montant (en euros) : ____________ Specify the amount of the reimbursement, in € : □ Versement d’une somme forfaitaire Lump-Sum payement : Préciser son montant (en euros) : ____________ Specify the amount of the lump-sum, in € : Le cas échéant, frais d’hébergement (cocher la case correspondante) : Lodging expenses (check the relevant box) : □ Prise en charge directe par l’employeur Directly paid by the employer : □ Remboursement des frais avancés par le travailleur Reimbursement of expenses advanced by the workers : Préciser son montant (en euros) : ____________ Specify the amount of the reimbursement, in € : □ Versement d’une somme forfaitaire Lump-Sum payement : Préciser son montant (en euros) : ____________ Specify the amount of the lump-sum, in € : DATE D’EXPIRATION DE L’ATTESTATION (au plus tard 6 mois après sa date d’établissement) Expiry date of the attestation (no later than six m onths after its issue) Date d’expiration (expiry date) : _______________________ Fait à _____________le _____________ Signed in , on Signature et cachet de l'employeur : Employer’s signature and stamp